





The active movements of the shoulder are provided by four tendons and associated muscles called the rotator cuff that combine humerus and scapula and move below the lower part of the acromion.
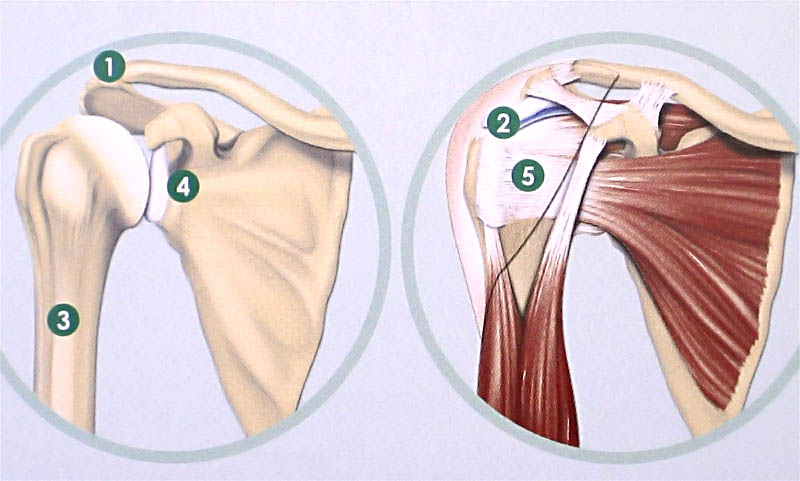
1 Acromion; 2 Bag subacromial; 3 Humerus; 4 Glenoide; 5 Rotator Cuff
Shoulder pain that radiates to the arm and increases with stress and / or at night is often the first symptom of the rotator cuff's pathology. In fact, already after 35-40 years old, it can begin a process of degeneration of the cuff's tendons characterized, after prolonged efforts and night's, by a loss of elasticity, microcalcifications with pain. There can establish an inflammation of the tendons and the subacromial bag, resulting in a framework of tendonitis or bursitis. In this phase the therapy is conservative (medical and rehabilitative), non-surgical and you can easily reach the healing. If the degeneration of the tendon becomes chronic, the rotator cuff can begin to wear thin against the acromial ceiling in the repeated movements with the limb elevated. There the chances of healing are reduced. Finally, if this process of degeneration and wear tendon persists (facilitated by any arthritic deformations of the acromion) or if there is a trauma to the shoulder, we reach the breaking of the rotator cuff. In this stage, once verified age, functional requirement and severity of the injury, the surgical treatment is applicable, which can be arthroscopic, open, or, in more severe cases, prosthetic.
The shoulder stability is due to the glenohumeral structures. When these structures become insufficient, traumatic episodes of dislocation take place or of structural laxity, this articulation becomes unstable, giving rise to the pathology that often takes the name of habitual dislocation of the shoulder. At this point the treatment, initially conservative becomes surgical: through arthroscopic or open surgical treatment the structures that have been damaged, or are insufficient to restore stability and function of the shoulder, are rebuilt.